


Cervical Myelopathy
Myelopathy describes any neurologic deficit related to the bone marrow not caused by an inflammation. When the cause is an inflammation, then the condition is called myelitis. Depending on the part of the marrow where myelopathy occurs, we distinguish it to be either thoracic or cervical myelopathy.
The most common cause of cervical myelopathy is the compression of the cervical bone marrow by any reason, such as a cervical disc herniation or a spinal canal stenosis that is usually caused by osteophytes formation and more rarely by the ossification of the posterior longitudinal ligament (OPLL).
Regardless of the cause of cervical myelopathy, its symptoms are always the same and depend on the extent of the bone marrow damage as well as the severity of myelopathy. Thus, in less severe cases of cervical myelopathy, patients complain about numbness in their hands and legs or the thorax that gradually worsen. In more severe cases of myelopathy, movement disorders occur (monoparesis, hemiparesis, or paraparesis), while in the most severe cases, mobility loss may be complete (monoplegia, hemiplegia, or paraplegia). Instability during walking can be manifested from the first stages of cervical myelopathy and is caused by the bone marrow nerve fibers’ compression (posterior funiculus) that transfer sensory signals relevant to balance and the limb’s position within a specific space (proprioception).
Finally, in the most extreme cases, cervical myelopathy symptoms include bladder or bowel incontinence and erectile dysfunction. Pain is not a common symptom of cervical myelopathy but it always accompanies cervical radiculopathy where compression affects both the cervical bone marrow and some cervical nerve root.
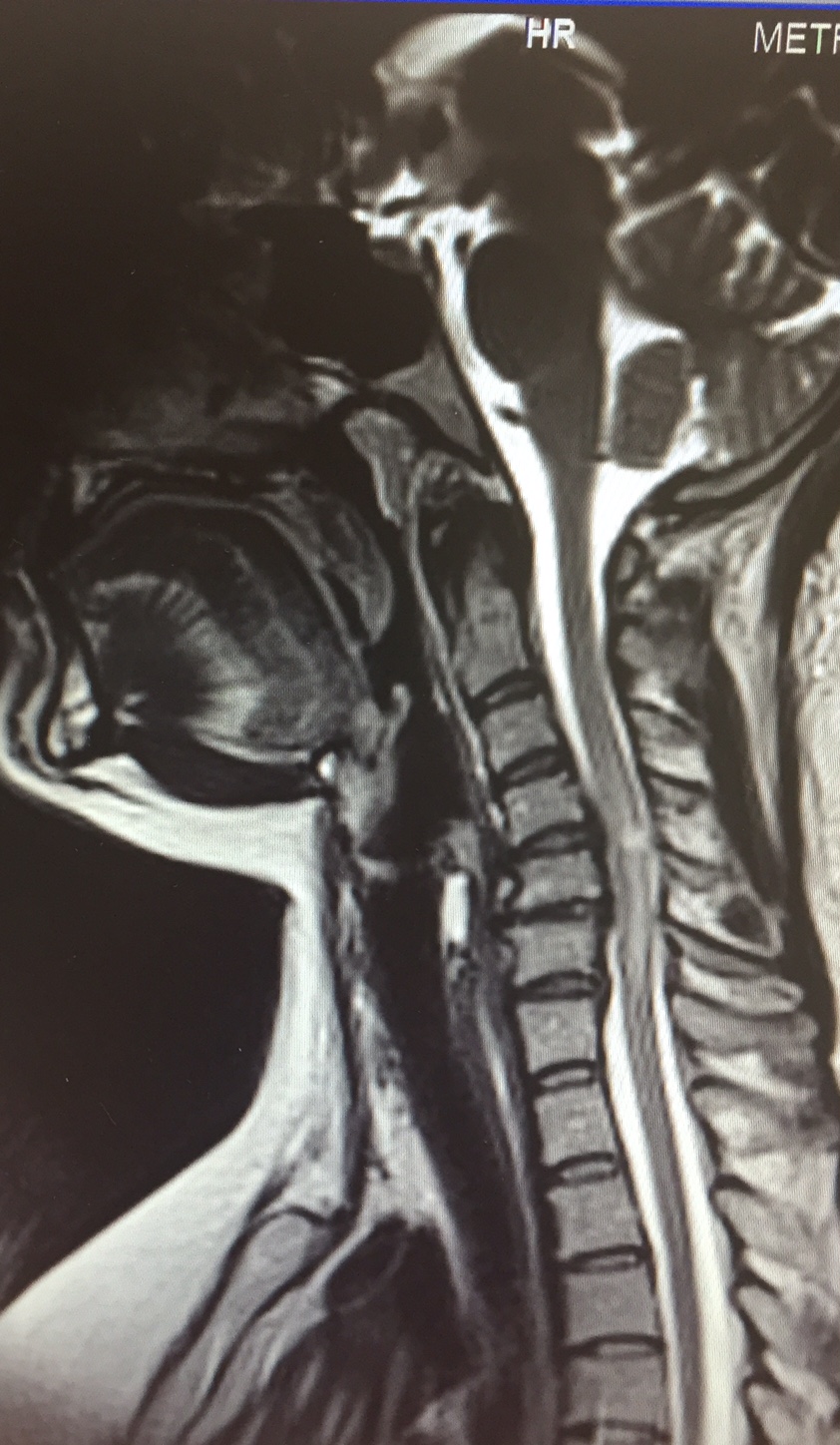
Cervical disc herniation, Α4–Α5 on the left side, with signs of compression and cervical bone marrow dislocation causing cervical myelopathy, as it is also depicted in the following image [Image taken from my personal archive]
Cervical myelopathy is usually diagnosed clinically by the neurologist or the neurosurgeon and is confirmed by a cervical MRI scan. Symptoms of cervical myelopathy are typical, such as the white intramedullary sign that shows the cervical bone marrow damage. With an MRI scan, we also identify the cause of the bone marrow compression, which is usually the treatment goal since the intramedullary damage cannot be reversed either with drugs or with a surgery.
For this reason, immediate surgical decompression of the cervical bone marrow should take place as this is the only way to prevent the progress of cervical myelopathy. The most important decompression techniques of the cervical bone marrow are applied either with anterior or posterior access. The first technique of the surgical treatment is chosen when movement disorders are more prevalent and this technique consists of cervical discectomy to one or multiple levels and spinal fusion with the use of materials (a fusion cage made of PEEK with or without a titanium plate) and bone implant. Posterior access is chosen when sensory symptoms are prevalent accompanied by instability during walking and it consists of laminectomy to one or multiple levels with or without spinal fusion with screws and titanium bars.
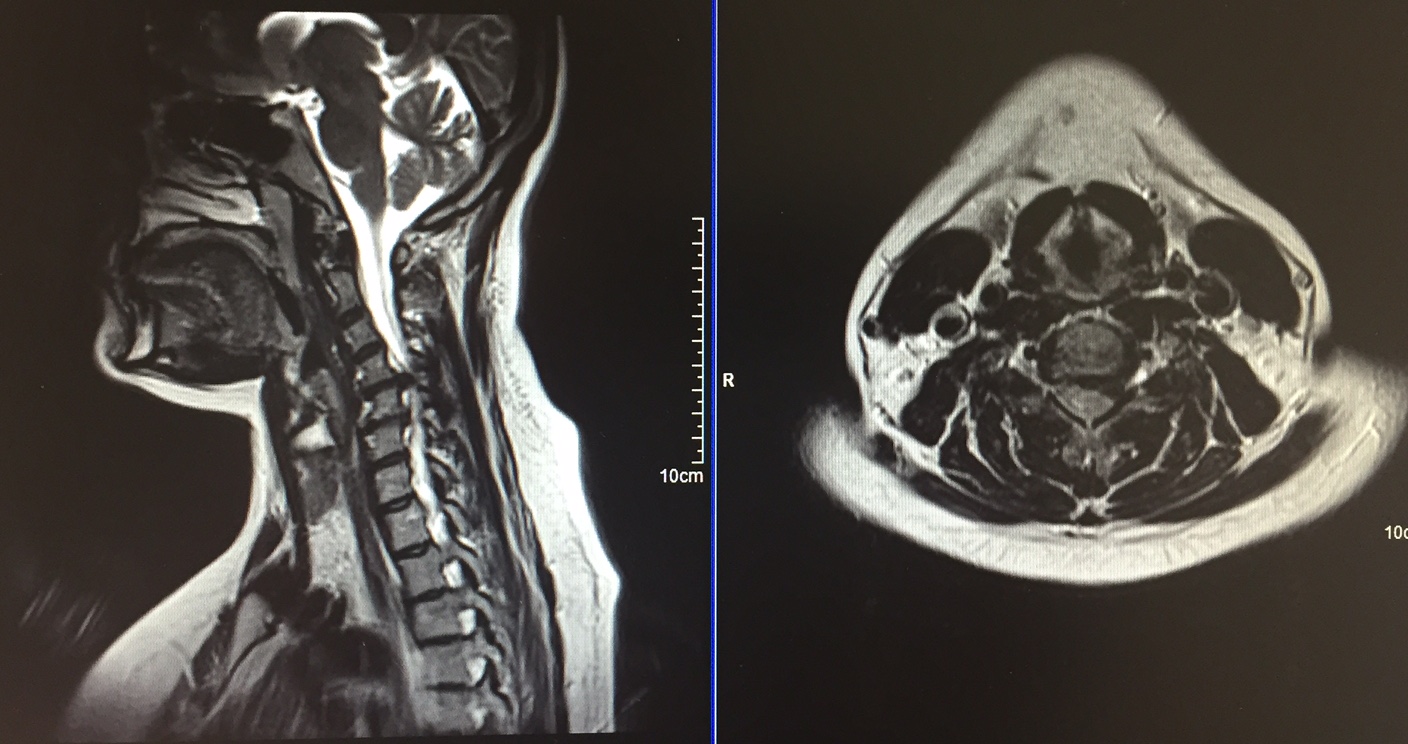
Ιntramedullary sign within the cervical bone marrow on a young female patient due to compression caused by a cervical disc herniation and spinal canal stenosis. [Image taken from my personal archive]
Unfortunately, pharmacotherapy can only help cervical myelopathy treatment in the improvement of the symptom’s severity (for example, baclofen improves spastic paraparesis). Physical therapy also helps but the results are extraordinary only after the surgical decompression of the cervical bone marrow, especially where there are movement disorders.



